Health Equity In India- Road To Ensure Access To All

Health is a fundamental human right enshrined in Article 21 of the Indian Constitution, yet access to it remains inequitable for millions in India. Health equity, as defined by the World Health Organization (WHO), is achieved when everyone has the opportunity to reach their full potential for health, free from disadvantages caused by social, economic, or political factors.
India faces significant disparities in healthcare access and outcomes between urban and rural areas. While metropolitan regions concentrate over 75% of the country’s healthcare professionals, rural areas face a critical shortage of healthcare professionals. Primary Health Centers (PHCs) in rural India are overwhelmed, catering to around 36,049 people each which is far exceeding their capacity and limiting access to quality healthcare. This strain is further aggravated by a critical shortage of human resources in many states (shown in fig 1). The number of doctors at PHCs decreased from 31,716 in 2021 to 30,640 in 2022, as reported in the Rural Health Statistics 2021-22. This shortfall significantly impacts rural community’s access to timely and adequate medical care, underscoring the urgent need for strategic improvements in healthcare staffing and resources in these areas.
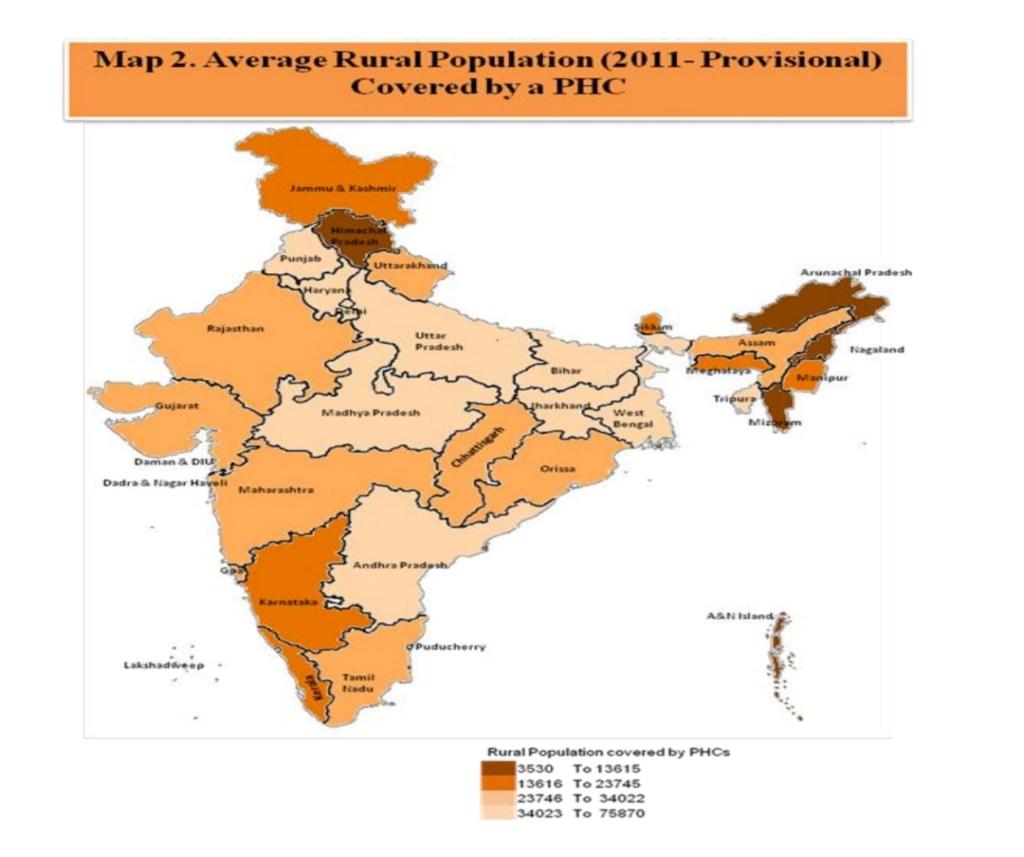
Fig 1 Source – National Rural health statistics 2021-22
Health inequities are stark among marginalised communities such as Scheduled Castes and Scheduled Tribes. National Family Health Survey (NFHS)-5 data shows that these communities have higher child mortality rates and lower immunisation rates. Tribal communities face significant health challenges due to inadequate access to nutritious food, resulting in hunger, stunting, wasting, anemia, and deficiencies in essential vitamins and minerals. They are also highly vulnerable to infectious diseases like malaria, tuberculosis, leprosy, HIV/AIDS, diarrhea, respiratory infections, and vector-borne illnesses, exacerbated by poor sanitation, limited healthcare access, and insufficient infrastructure. Moreover, there is a very limited presence of doctors, nurses, and healthcare professionals in tribal regions.
Gender inequality manifests in profound ways in India, where women in poorer, marginalised communities face higher health risks. Access to healthcare for women, particularly reproductive and maternal health services, is limited by both social norms and economic constraints, hindering their ability to achieve optimum health outcomes. Currently, over half of the children and women (including pregnant women) are anemic across all Phase-II states/UTs and at the national level, showing an increase compared to NFHS-4. The prevalence of anemia among women increased from 53.1% in NFHS-4 to 57% in NFHS-5, highlighting a concerning trend. Additionally, the significant disparity in anemia rates between men and women (as depicted in the figure below) underscores the persistent health inequities.
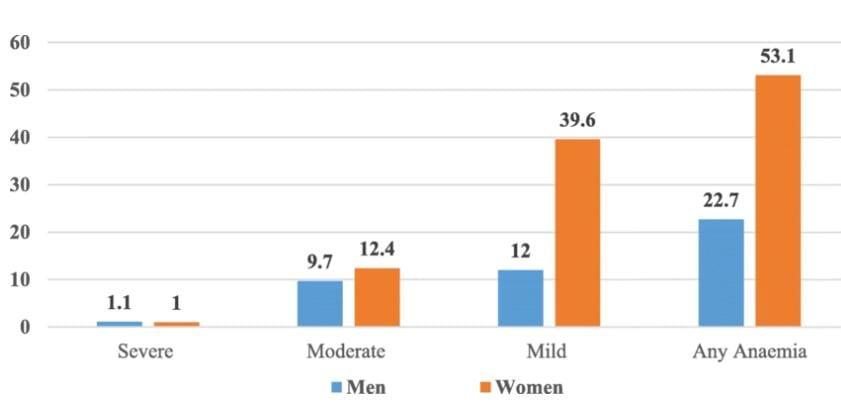
Fig 2 Source- NFHS 2015- 2016; Prevalence of anaemia in men and women between age of 15-49
One of the primary challenges in achieving health equity is the high out-of-pocket expenditure (OOPE) that continues to push nearly 39 million people into poverty annually. In India, households bear over 75% of rising healthcare costs, creating a severe economic burden for low-income families. National Family Health Survey 5 (NFHS) indicates that the Out-of-pocket expenditure (OOPE) per delivery in a public health facility at all-India level is Rs. 2,916. Health insurance has emerged as a financing option in India to tackle out-of-pocket expenses, though it remains underdeveloped compared to developed countries. However, 40 crore individuals (referred as the missing middle in fig 3 below) are devoid of any financial protection for health.

Fig 3 Source – Niti Ayog’s Health Insurance for India’s Missing Middle Report
The road to ensure health equity in India
To ensure health equity, India should focus on achieving Universal health coverage by strengthening Primary Healthcare as recommended by Srinath Reddy Committee’s 2010 report. It emphasizes that the government allocates at least 70% of health funds to strengthen primary healthcare, the foundation of the healthcare system, ensuring access to essential medicines and basic services for all. Even, WHO recognises primary care as essential for promoting health equity and achieving universal health outcomes, backed by substantial theoretical and empirical evidence. Countries with robust primary care systems tend to have better health equity and outcomes. India should replicate successful primary healthcare models, such as Telangana’s Basthi Dawakhanas and Kerala’s Family Health Centres, in other regions to strengthen its healthcare framework.
Fig 4 Source – WHO
Furthermore, expanding health insurance is essential to achieving health equity in India. There is need to establish more inclusive health insurance policies to reduce OOPE and protect vulnerable populations from catastrophic health expenditures. Policies should target rural and marginalized populations, ensuring equitable financial protection. Developing a modified, standardized health insurance product like ‘Aarogya Sanjeevani’ can be a transformative solution.
Technology can be leveraged for enhanced Healthcare Delivery to underserved areas. Model digital health centers should be established with a minimum staffing of one MBBS doctor, supported by a pharmacist and an IT operator. Additionally, affordable drug delivery can be achieved by integrating the government’s Jan Aushadhi Yojana with an e-pharmacy initiative, potentially through partnerships with platforms like 1mg and Netmeds, to improve access to low-cost medications. Leveraging healthcare technologies, such as indigenous medical devices, diagnostics, telemedicine, AI tools, and drones, could greatly improve accessibility, affordability, availability, and health awareness, ultimately narrowing healthcare disparities and enhancing well-being across India. Artificial Intelligence (AI) contributes by analyzing large data sets to improve diagnostics and treatment options, which can alleviate the workload on healthcare professionals. In remote tribal regions, drones offer an efficient means to deliver essential medications, while the Internet of Things (IoT) enables connected health monitoring devices, providing valuable insights into patient health.
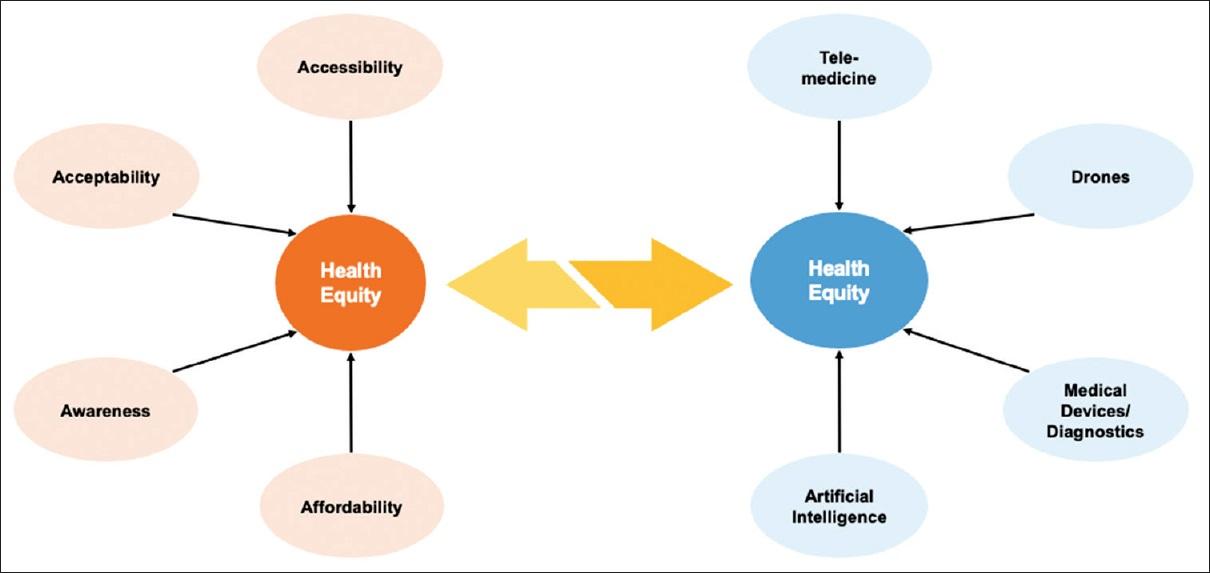
Fig 5 – Source Gupta et al
In conclusion, achieving health equity in India requires a multifaceted approach that addresses the existing gaps in healthcare access, affordability, and resource distribution. Leveraging technology through telemedicine, AI, and the Internet of Things (IoT) can play a transformative role in bridging the urban-rural divide, improving healthcare delivery in remote areas, and providing real-time patient insights. To build a health system that serves all Indians equitably, concerted efforts are needed at both the union and state levels, in partnership with private sector initiatives, to ensure that health as a fundamental human right is accessible to every individual, fulfilling the promise of Article 21 and creating a pathway toward universal health coverage.
Register your Interest to Study at ISPP
References –
- Gupta, P., Choudhury, R., & Kotwal, A. (2023). Achieving health equity through healthcare technology: Perspective from India. Journal of Family Medicine and Primary Care, 12(9), 1814–1817. https://doi.org/10.4103/jfmpc.jfmpc_321_23
- Balarajan, Y., Selvaraj, S., & Subramanian, S. (2011). Health care and equity in India. The Lancet, 377(9764), 505–515. https://doi.org/10.1016/s0140-6736(10)61894-6
- The People’s Archive of Rural India. (n.d.). Rural Health Statistics, 2021-22. People’s Archive of Rural India. https://ruralindiaonline.org/en/library/resource/rural-health-statistics-2021-22/
- Kumar, A., & Sarwal, R. (2021). Health insurance for India’s missing middle [English]. In NITI Aayog, NITI Aayog. https://doi.org/10.31219/osf.io/s2x8r
- World Health Organization: WHO. (2021, July 7). Health equity. https://www.who.int/health-topics/health-equity
- Nation family health survey 5, 2019-21
- National family health survey 4, 2015-16

Shivani Patel
PDM Scholar, Class of 2025
Shivani Patel, hailing from a small village in Madhya Pradesh, is a scholar of the current PDM Batch at ISPP. She aspires to transform the lives of millions through impactful work in the health and education sector. As a graduate of Political Science, Public Administration, and Sociology from Banasthali University, her academic journey reflects her unwavering dedication to understanding societal challenges and finding actionable solutions. She has actively participated in various national-level youth parliaments, MUNs, and debate competitions, earning accolades for her performances.
Shivani’s experience as a former UPSC aspirant has provided her with deep insights into governance and policymaking. At ISPP, she initiated the ‘Policy Sabha’ to foster meaningful policy discussions among scholars. She recently joined Change Engine as a Research Intern, where she is involved in studying non-profit unicorns. Shivani envisions bridging policy and grassroots action, driving sustainable change to uplift underserved communities across India.
LinkedIn: https://www.linkedin.com/in/shivani-patel-0794a1315/